
The Centers for Medicare & Medicaid Services’ (CMS) recently proposed Value-Based Purchasing Program updates include staffing provisions that are being met with provider concern, although other updates should be well received once the dust settles.
Among recommended changes, CMS is proposing allowing SNFs to review and correct Payroll-Based Journal (PBJ) data beginning with the fiscal 2026 program year.
Given that there was no further guidance on how the federal government’s staffing mandate aims to be fulfilled, providers who spoke to Skilled Nursing News said that having this ability to correct and review PBJ data will not achieve anything. Moreover – particularly in light of current staffing challenges and the looming, unfunded federal mandate – they are pushing back on the inclusion of staffing measures that are set to take effect in the VBP program in fiscal year 2026, such as the total nursing staff turnover measure.
“I do not think that adding retention or PBJ measures to VBP is good for SNFs,” said Tiffany Beall, senior director of clinical reimbursement at ML Healthcare. “We are affected by PBJ or staffing in general, first and foremost, because we need trained staff to care for our residents who are increasingly having higher acuity [needs].”
ML Healthcare operates skilled nursing facilities located throughout Texas.
And besides not having enough staff, having staff with the right skill set requires providers to pay higher wages, she said, which CMS’ proposed SNF payment rate for 2025 doesn’t enable.
However, another proposed change to the VBP program could be better news for providers.
That proposal is for a “measure selection, retention, and removal” policy to begin with fiscal year 2026. This policy would set a firmer framework similar to the one in the SNF Quality Reporting Program (QRP), to create a greater sense of certainty around which measures will be considered in value-based purchasing and how measures would be removed.
PBJ’s link to VBP is complicated in some states
Another problem stems from PBJ’s inclusion in the Quality Incentive Payment Program (QIPP) in Texas, Beall pointed out. PBJ will be used to assess whether a QIPP-eligible facility qualifies to receive incentive payment based on staffing levels. The Texas Health and Human Services Department may validate use PBJ data to validate whether a facility met mandated RN hours.
In other words, the increasing interrelationship among PBJ, incentive payment programs and the Five-Star system creates a web of data that can influence referrals and census numbers and, of course, revenue.
“PBJ has also moved to the QIPP program, which will affect the potential for SNFs to help bring in the revenue needed to pay for the staff they need,” Beall said.
Beall is planning to weigh in before CMS finalizes the SNF PPS rule to advise that the federal agency move to a different type of change.
“I will likely comment and suggest that instead of adding PBJ, they look at changing the methodology used to calculate the rates currently. Why can we not look at residents as people instead of diagnosis codes and days they need to recover,” she said. “Every person is different and should be treated as such.”
Measures policy allows for stability
The SNF VBP Program allows CMS to award incentive payments to SNFs to encourage improvements in the quality of care provided to Medicare beneficiaries. The agency is statutorily required to include a SNF readmission measure, but is allowed to apply up to nine additional measures related to areas such as functional status, patient safety, care coordination and patient experience.
In its 2025 proposed SNF rule, the federal agency is intending to improve alignment of measures across its quality programs so as to reduce burden on providers.
And to that end, CMS is also recommending adopting a measure retention and removal policy. It plans to create a “Universal Foundation” of quality measures across its quality reporting and value-based care programs, with additional measures added depending on the population or setting, which the federal agency refers to as “add-on sets.”
For Aaron Kirkman, senior analyst in ATI’s Value-Based Care Design and Delivery Practice, the biggest updates – via the proposed measure retention and removal policy – will allow for stability and should be a welcome move by nursing homes.
The language of the proposed SNF rule is detailed enough to suggest that CMS intends to stabilize the process.
“They’re kind of finalizing the list of measures that they’re going to have in VBP for the next probably two or three performance years. They’re proposing to put in place this official policy around the selection, retention and removal of the VBP measures,” said Kirkman. “[CMS is] saying, ‘Once we add a measure, it’s going to be added for the foreseeable future. We’re not going to remove it. If we do choose to remove it, here are the criteria that we’ll use to decide whether to replace or remove a measure.’”
Indeed, the proposed rule states that when a measure is adopted for the VBP program, it would “automatically be retained for all subsequent years” unless CMS specifically proposes to remove or replace it. This policy would mean the agency would not have to “continuously propose” a measure for inclusion year after year.
The proposed rule includes eight specific factors that would be weighed when determining whether a measure should be considered for removal or replacement. As laid out in the proposal, considerations would include uniformly good performance across a measure, signaling that “meaningful distinctions and improvements in performance can no longer be made”; and whether improvement on a given measure is helping resident outcomes.
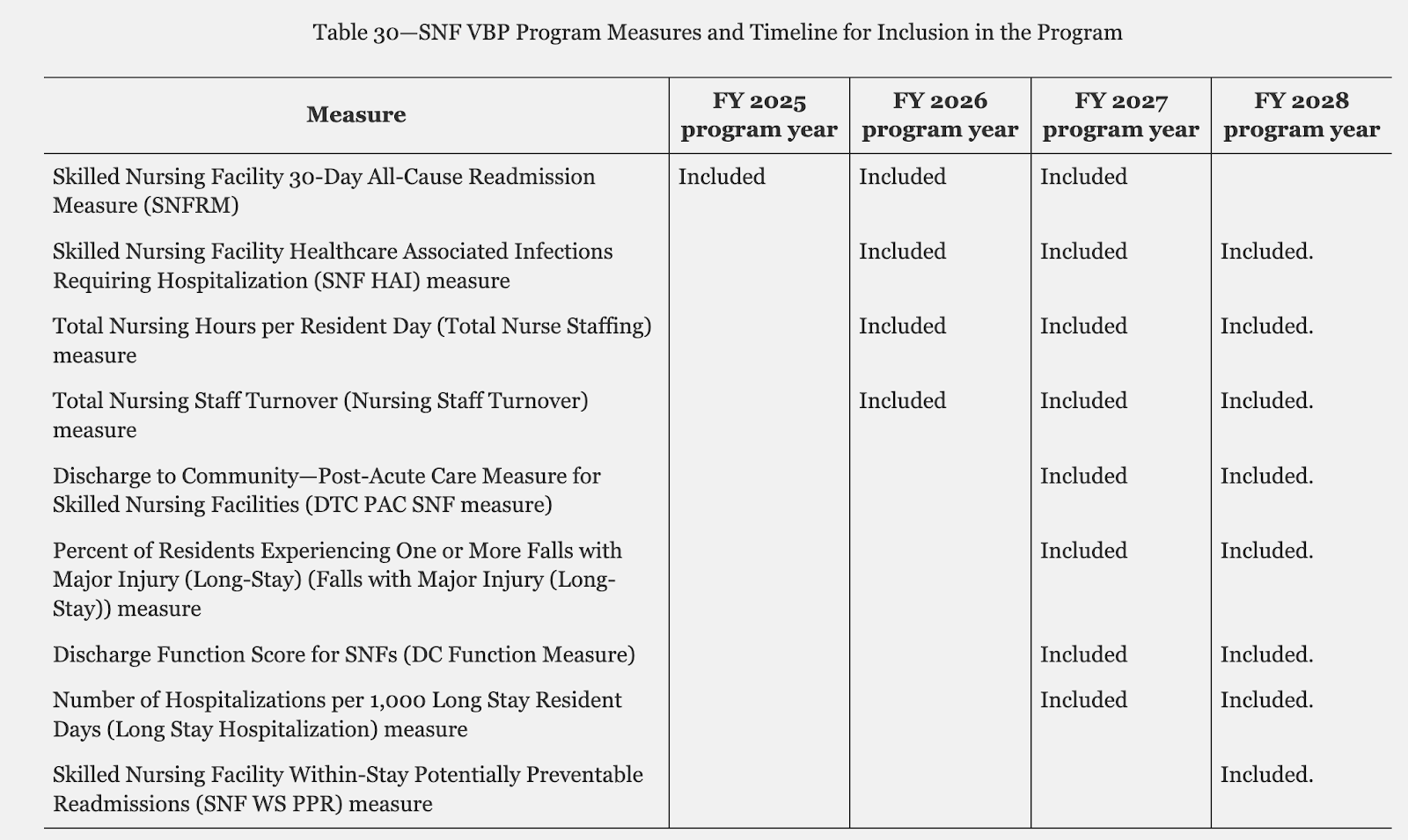
Source: CMS
“And so now that we have this policy in place, the big takeaway is that, okay, those measures are here to stay. And if there are circumstances where those measures will be removed, it’s not going to be an overnight thing unless a measure is harming residents,” Kirkman said.
And this aspect of the VBP updates should be well received once it’s all said and done.
“I would expect that any stability is welcome. Now, of course, that begs the question of, are the exact measures welcome? But, there are always some [critics]. Nobody’s completely in favor of every measure. So I expect that’ll stay the same,” Kirkman said.
As for what specific measures CMS might propose for inclusion in the VBP program, he points to the agency’s overarching priorities related to “ interoperability, health equity, social determinants of health” as good clues.
The agency flagged its intentions related to these areas within the proposed rule, noting “several resident experience measures” that are being assessed.
CMS also is considering whether a composite staffing measure is feasible, which would combine the two separate staffing measures in the current set.
Public comments are being gathered in response to the proposed rule through May 28.
Companies featured in this article:
ATI Advisory, Centers for Medicare & Medicaid Services, CMS, ML Healthcare
