Conspicuously absent data on Medicare Advantage (MA), along with stagnated data collection overall by government agencies, should give nursing home operators cause for concern especially as this trend has influenced company advocacy and negotiating power when it comes to insurance plans.
Having this data and understanding how it’s calculated can help operators “speak the same language” as the insurance companies when negotiating rates, according to Marc Zimmet, president of Zimmet Healthcare Services Group.
Concerningly, the Centers for Medicare & Medicaid Services (CMS) is now asking nursing home providers to help them capture data to drive MA reports, said Zimmet. This should not fall under the responsibility of nursing home operators, he said.
“That’s their job [but] CMS does a horrific, horrific job at this. They should be ashamed of themselves. [The Medicare Payment Advisory Commission] MedPAC should be ashamed of themselves in terms of how they’ve let skilled nursing data atrophy to the point where it’s borderline useless,” Zimmet said.
To improve data collection, Zimmet said that CMS could change a “title,” or a section in its Medicare cost report, from maternal and child care benefit to Medicare Advantage as a category to monitor, but it hasn’t.
“This is a vestige from the fifties when I suppose these risk averse facilities provided a different type of care,” said Zimmet during a webinar on Tuesday. “All Medicare needs to do, all CMS needs to do, is to change that Title V to Medicare Advantage, and we’d have good data.”
Meanwhile, MA enrollees jumped from about 7 million in 2006 to 28.8 million 2022 to meet traditional Fee-for-Service Medicare, which had 29 million enrollees in 2022.
MA plans are using Hierarchical Condition Coding Risk Adjustment Factor (HCC-RAF) scoring to calculate per member per month rates, said Vincent Fedele, who serves as partner at Zimmet Healthcare and COO of z.PAX, the Post Acute eXchange. It’s similar to case mix, he said.
The higher the score, the higher the payment, and there’s different models for different care settings. It’s the Medicare Advantage Organizations’ (MAO) way of filling the gap left by CMS when it comes to data collection for this rapidly growing population.
Scores are calculated using a combination of demographics like sex, age, location, their original eligibility for Medicare and acuity too.
“The HCC codes are accretive. It’s not an index maximizing type system like we’re familiar with in the nursing component of our PDPM system,” said Fedele. “It’s more like the non-therapy ancillary where the codes get added together to produce a risk adjustment factor at the plan level, based on how the data is submitted for those plans.”
Zimmet used Medicare average length of stay as an example of gaps in government data for nursing homes, with data from the claims domain and cost report not matching up. The analysis found a difference of just under 10 days in this statistic between 2014 and 2020.
Zimmet broke down eight different data domains for nursing homes, three of which are protected in some way by the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule or private health information – that’s financial documents, the Minimum Data Set (MDS) and electronic medical records.
Accessible data domains include the Payroll Based Journal (PBJ), Care Compare, Standard Analytic Files (LDS-SAF) claim data, the Healthcare Cost Report Information System (HCRIS) database, the national health safety network and CMS files.
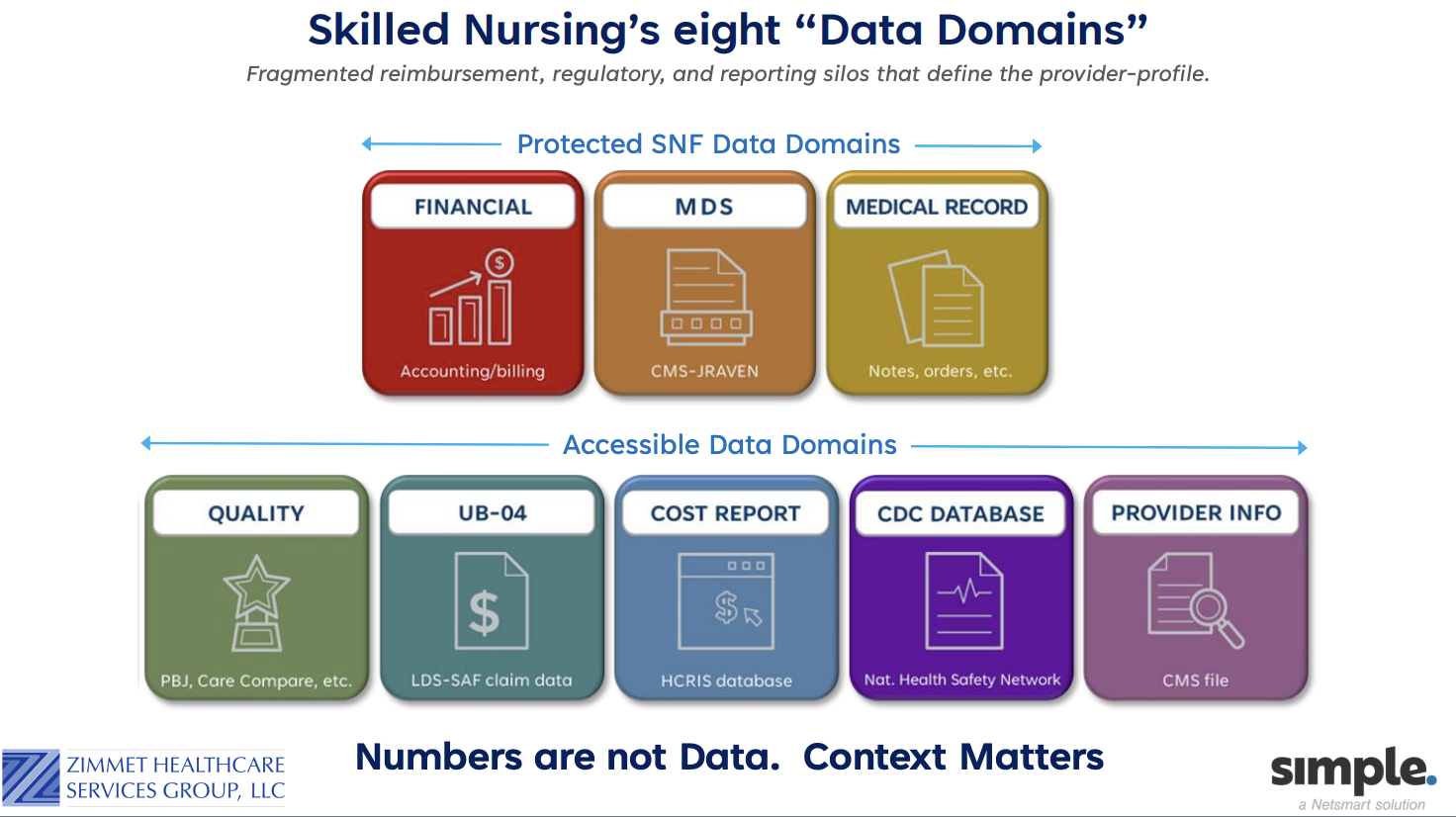
But, accessible doesn’t mean readable, he said, and raw data needs to be deciphered and put into context.
“There’s a whole world of data out there. It’s defining each facility … every facility out there has got their own data profile. It’s critical that you understand the data that’s being presented about you and what it means,” said Zimmet.
Companies featured in this article:
Centers for Medicare & Medicaid Services, CMS, Zimmet Healthcare Services Group
