Skilled nursing providers might be able to reap financial gains under the new Medicare payment model taking effect in October of this year if they can cut their average patient length of stay (LOS).
But the gains will only hold until a certain point, and providers that already have shorter LOS —- such as short-term rehab facilities — might find that the risks outweigh the rewards.
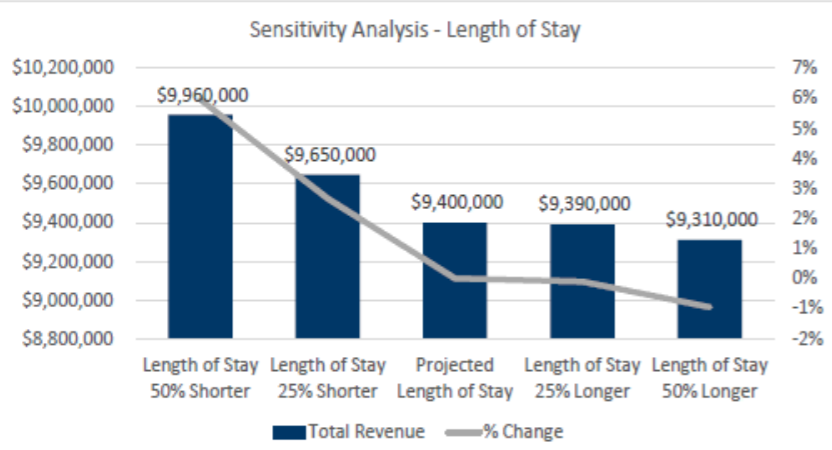
A Tuesday webinar on the financial implications of the Patient-Driven Payment Model (PDPM), held by the professional services firm CliftonLarsonAllen, explained why. Under PDPM, the physical and occupational therapy rate components have a variable per-diem adjustment, dropping by 2% every seven days after day 20 of a given SNF stay. The non-therapy ancillary (NTA) component also has a variable per diem adjustment, with that portion after three days declining by 67% until discharge.
That means that if SNFs are able to keep the LOS close to 20 days, they will get the highest rates and continue to get paid at those rates. But that depends on keeping their census steady the presenters noted.
“If your LOS is over 20 days, your average LOS, and you can shorten that with the assumption that you can keep your total census the same — and I know that’s a challenge, and that’s a big assumption to make in the analysis — but if you can do that, there is the potential to pick up additional revenue,” Deb Freeland, principal in CLA’s health care practice, said on the webinar.
For providers with a shorter length of stay, however, this could be a challenge that isn’t worth the aggravation. Several SNFs have moved to a focus on high-acuity, short-term rehab over the years, to the point that US News & World Report — and more recently the Centers for Medicare & Medicaid Services (CMS) — have rolled out separate ratings systems for short- and long-term focused SNFs.
But the problem for these SNFs is that there isn’t as much opportunity to pick up additional revenue if a SNF is already at a 20-day average LOS or even below, Freeland noted.
“You then run into the challenge of your ability to keep your census where it should be,” she added. “And so you really have to look at your own individual facility and what your LOS is to figure out what that potential impact could be.”
LOS pressures have come into focus in recent years as new alternate payment models — from Medicare Advantage to accountable care organizations — demand shorter stays to reduce overall episodic costs. Accounting and advisory firm Plante Moran, for instance, found that average Medicare lengths of stay dropped from 40 days to 38 days between 2016 and 2017, and clocked in as low as 35 in certain markets. But for Medicare Advantage patients, that average amount typically falls around 20 days or fewer, lining up with CLA’s analysis.
Despite questions about therapy provision under PDPM, facilities that provide high amounts of rehabilitation aren’t necessarily going to be losers under PDPM, Freeland noted on the webinar.
“You really need to look at the whole picture and what are you potentially missing on the MDS, what are you missing on the ICD-10, that could positively impact your facility,” she noted.
Hilary Forman, the chief clinical strategies officer for the consulting firm HealthPRO Heritage, which provides rehab services among others, agreed. Therapy has a major opportunity to consider different ways of providing services under PDPM — methods that aren’t minutes-focused, she said. Rehab providers might also be involved in different ways in a facility or organization’s post-acute strategy, such as assistance with care management, designing clinical pathways, or looking at overall education, even in areas such as nursing or non-therapy ancillary components.
“There’s a lot of upside opportunity in PDPM, from a therapy perspective,” she said.
But providers need to be exceptionally wary of drastic changes in behavior, Forman noted, since cutting rehab hours could be a compliance risk and affect patient satisfaction, outcomes and a facility’s preferred provider status adversely. But the need to be careful of major changes isn’t confined to the therapy and rehab front, where CMS has warned there will be scrutiny.
PDPM is intended to be budget-neutral, meaning that CMS won’t be changing the amount it spends on skilled nursing care as a result of the change. While Freeland joined others in arguing that behavior changes at an organization will include more focus on the accurate completion of Minimum Data Set (MDS) assessment, it’s not clear how that will play out for providers.
“What are those behavior changes going to do to that budget neutrality from CMS’s perspective?” she asked rhetorically. “I think that’s something we need to continue to watch and monitor as PDPM is implemented.”
