
SNN presents this guest analysis from Anne Tumlinson and Elizabeth Walsh of Anne Tumlinson Innovations.
Health care providers selling Medicare Advantage (MA) products isn’t a new trend, but typically “providers” refers to hospitals, health systems, or physician groups. Few would expect nursing homes and assisted living operators to be able or willing to manage health care risk for some of the highest-cost Medicare beneficiaries.
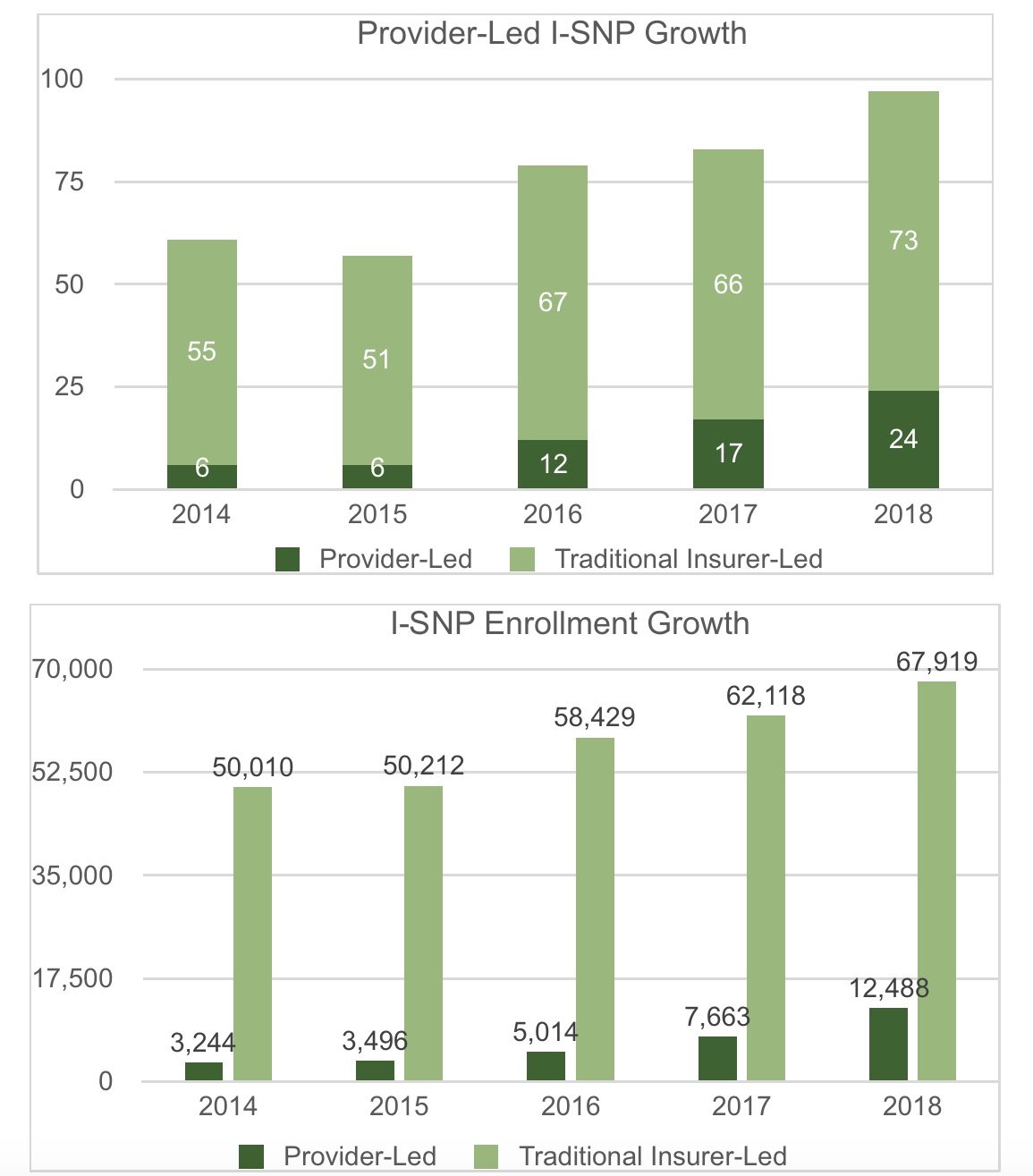
And yet, as these charts illustrate, long-term care providers are largely responsible for driving rapid growth (23%) in the number of MA special needs plans enrolling institutionalized Medicare beneficiaries over the last two years. The number of provider-sponsored I-SNPs doubled from 2016 to 2018, and enrollment has more than doubled. Long-term care providers now lead 21 of the 24 provider-led I-SNPs.
Why is this happening? Our team spent the last year traveling around the country talking to long-term care providers who are operating plans and educating facility operators. Here’s what we learned.
Many nursing home operators view healthcare risk models as the only viable business path forward.
Nursing home operators tell us the traditional nursing home business model — where margin depends solely on volume and daily rates — is becoming unviable. Nursing facilities have long expressed concern about sufficiency of Medicaid rates to cover costs of care; but in the past, they have generally been able to operate at positive and sustainable overall net margins thanks to sufficient short-stay patient volume in higher-reimbursed fee-for-service (FFS) Medicare.
Now skilled nursing facilities face a combination of business challenges, specific to higher-reimbursed Medicare admissions. Referring inpatient hospital volume has been declining and enrollment in MA is growing. MA plans tend to pay lower daily rates and more tightly manage length of stay. Even seemingly high performers complain that they have insufficient market leverage to secure value-based contracts from accountable care organizations (ACOs) or health plans.
Many operators see taking on health care risk – through bundled payments, SNPs, or in a few instances ACOs – as the only option for gaining more control over their financial future and capturing the savings from reduced hospitalizations, shorter stays, and coordinated transitions.
I-SNPs can provide nursing homes and assisted living with the financing for much needed primary care and care coordination.
Today’s I-SNP, now a permanent part of the Medicare program, originated from a demonstration of the EverCare model, in which onsite nurse practitioners deliver care aimed at reducing unnecessary hospitalizations. The provider-owned I-SNP gives nursing home operators direct Medicare funding – through the premium — to finance robust onsite primary care and care coordination for the long-stay resident population. It also rewards providers for the avoidance of long-stay resident hospitalizations whereas perverse incentives in the FFS system reward facilities that hospitalize long-stay residents.
Facility settings can support effective care management.
Facility operators have discovered that they have, in abundance, what ACOs and insurers only dream about: The ability to observe a complex care population in their “home” environment, to observe them frequently, and to manage health care for many high need individuals in one location. Nursing home and assisted living operators find that they do not need the large enrollment numbers of typical MA plans because the facility setting supports strong care management. The average enrollment for provider-led I-SNPs is about 520.
Most LTC-owned plan leaders with whom we speak tell us that they are managing health care spending within the medical loss ratio, and sharing savings with the network providers who are contributing to a reduction in high-cost health care.
Many of these providers contract with the Centers for Medicare & Medicaid Services (CMS) with the help of partner organizations that bring insurance and compliance expertise. Despite this administrative help, there are still many challenges that providers must overcome in forming and operating a SNP, including licensure and reserve requirements, forming provider networks, and recruiting and training nurse practitioners.
As the provider-led I-SNP trend grows, policymakers are inevitably going to raise questions. They will want to know if I-SNPs impact nursing home quality measures. What happens to care for residents who do not enroll? Should we be concerned about enrollment practices or selection bias?
CMS will certainly begin to examine this trend alongside and within the larger context of MA program growth, provider-led risk arrangements, and the need to find platforms that support integration of acute and long-term care. Time – and data — will tell if the provider-led I-SNP is here to stay; but for more and more long-term care providers, it is an opportunity to stay in the game.
Anne Tumlinson is the founder and CEO of health care consulting and advisory firm Anne Tumlinson Innovations. Elizabeth Walsh serves as ATI’s lead content strategist and consultant.

{kind=link}